Nevada has one of the lowest rates of colon cancer screening
Reviewed by Dr. Craig Sande
Here’s the truth: a colonoscopy is the only cancer screening tool that can actually prevent the disease.
But, we still believe the best test is the one that you or your friend, spouse or family member will get done.
In Nevada, those screening tools are simply not being used as adequately as they need to be.
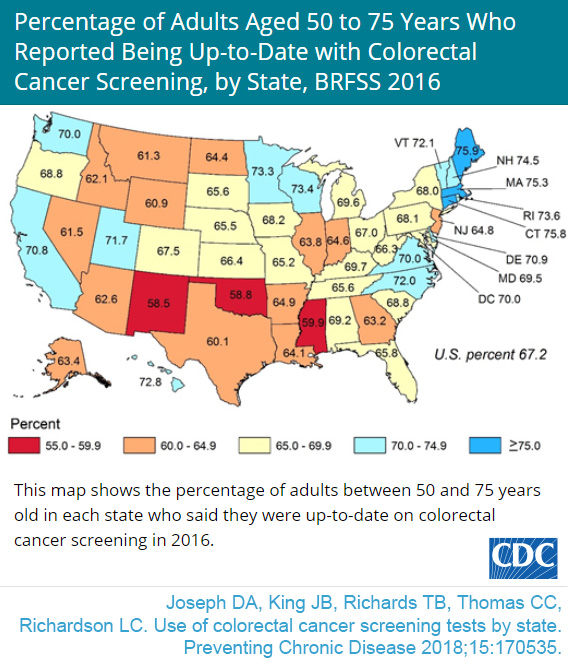 The Silver State ranked in the lowest ten states across the country for screening rates during 2016, which includes either a fecal blood test, a sigmoidoscopy or a colonoscopy, according to the Centers for Disease Control and Prevention. This means Nevada falls at seventh place for lowest screening rates, at just 61.5 percent of all adults over the age of 50 getting screened for colon cancer.
The Silver State ranked in the lowest ten states across the country for screening rates during 2016, which includes either a fecal blood test, a sigmoidoscopy or a colonoscopy, according to the Centers for Disease Control and Prevention. This means Nevada falls at seventh place for lowest screening rates, at just 61.5 percent of all adults over the age of 50 getting screened for colon cancer.
We barely squeeze in front of Montana (61.3 percent) and Wyoming (60.9 percent).
On the other hand, the incidence of colorectal cancer for Nevada ranks above the national average, as do the state’s colon cancer-related mortalities.
“Colonoscopies shouldn’t be feared – not when the benefits so far outweigh the drawbacks.” said Craig Sande, MD. “So many people say they are worried the colonoscopy will be painful, but usually they won’t have any recollection the procedure even happened.”
You probably won’t experience any symptoms when polyps start to grow in the colon, Dr. Sande said. However, the masses can turn into cancer if left untreated.
This is why colonoscopies are considered the gold standard of cancer screening. Unlike the Fecal Immunochemical Test, which checks for blood in the stool, colonoscopies allow doctors to see inside the colon and remove any growths before they become too large.
Regular screening should begin at age 50 for average-risk individuals and be continued every 10 years until age 75 – unless otherwise directed by a physician. Individuals age 76 to 85 should ask their doctor if they should be screened.
It is important to notice that you may need to begin screening earlier if:
- You have a close relative who had colorectal polyps or colorectal cancer.
- You have inflammatory bowel disease, such as Crohn’s or ulcerative colitis.
- You have a genetic syndrome, such as hereditary non-polyposis colorectal cancer, that would make you more inclined to develop colorectal cancer.
- Fecal immunochemical test (FIT): This test checks the stool for tiny amounts of blood given off by polyps or colorectal cancer. Remember, this type of test could produce a false-positive if blood is present in the stool for any other reason, such as hemorrhoids. It must be performed on an annual basis.
- CT colonography: This involves a CT scanner and computer programs to create a three-dimensional view of the inside of the colon and rectum that can be used to identify polyps or cancer. While this cannot remove polyps, it is fairly quick and noninvasive. However, it works best for large polyps.
- Cologuard: This tests the stool for tiny amounts of blood and identifies altered DNA from cancer or polyps that end up in the stool. While Cologuard™ is noninvasive, it will miss most polyps. The test comes with a high chance of false-positive results.
To schedule your colonoscopy or to discuss other digestive health needs, please reach out to Dr. Craig Sande or one of our other physicians at three locations throughout Reno and Carson City.
Dr. Sande is a Reno native and the fifth of six children raised by Naomi and John Sande. Medicine was not exactly the career path he had in mind when he left Reno to do his undergrad at Stanford University. He initially considered a career in electrical engineering, but after further exploration, he decided to follow his father’s footsteps and entered the field of medicine. Dr. Sande has a special clinical interest in inflammatory bowel disease, such as Crohn’s disease and ulcerative colitis, gastroesophageal reflux disease and esophageal motility disorders.